
Training Packages and Patient Management Tools for Healthcare Staff Working with Small, Nutritionally At-Risk Infants Aged under 6 Months: A Mixed-Methods Study †

.jpg)

Abstract
:1. Introduction
- To improve the future management of small and nutritionally at-risk infants and their mothers via an improved understanding of currently available training packages and patient management tools.
- To identify how many training programs and tools are currently available and their differences.
- To identify perceived issues and gaps in the practical application of training.
- To identify how training can be improved to ensure optimal delivery.
2. Methods
2.1. Study Design
2.2. Review of the Literature
2.3. Qualitative Research
2.3.1. Participant Selection
2.3.2. Data Collection
2.3.3. Data Management and Analysis
2.3.4. Ethical Considerations
3. Results
3.1. Identification of Training Programs and Patient Support Tools
3.2. Interviews
3.2.1. Participant Profile
3.2.2. Training and Management Tool Characteristics According to Key Informants
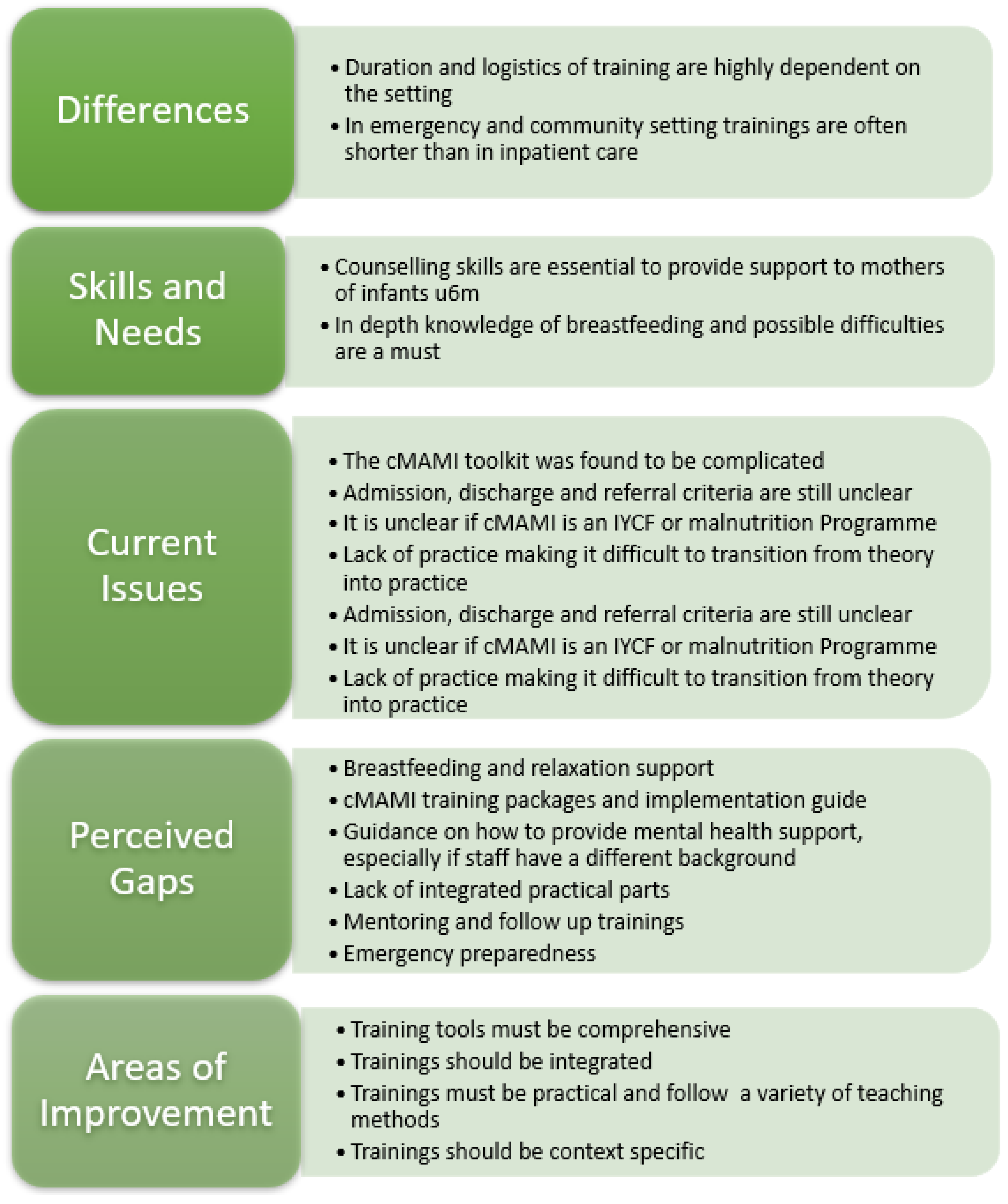
3.2.3. Themes Arising
3.2.4. Skills and Needs
“Because it is actually really important to get the technical knowledge for the staff but actually if they don’t know how to do counselling and I have seen it in so many different countries, then it is not gonna be successful.”ID3
“…they know it is the best thing for the baby, but they have too many other problems and so listening to those other problems I think is important.”ID9
“I mean, skills are one thing but really engaging with people’s attitudes and values (…) think we neglect that part (...) I mean for example in lot of what we are talking about are differences in life and death, so it is about how do you take the responsibility for that role and what does that mean to you as a person, why are you motivated to do this job, that kind of stuff.”ID2
“…especially when it comes to helping with breastfeeding which is a lot of (...) in the dark, you need to understand malnutrition and you need to understand about breastfeeding and also a little bit about how you can spot a preterm baby. I mean a lot of those babies are actually not malnourished, but they are born preterm unless you know the gestational age of the baby then you label it as malnourished.”ID2
3.2.5. Perceived Issues and Gaps
“There was a little bit of practical on it, but with the extent of this one-day orientation the team does not feel confident to then cascade it down when I was checking last week. And this is from some who are experienced in IYCF and acute malnutrition.”ID8
“…it is still heavily NGO-supported because we made it a bit too complicated and if we keep changing the admission and discharge cut offs, because this is what happened with CMAM, it’s gone from weight for height to weight for age and then it is three MUAC cut offs now it’s got two, you know you can only do a certain amount of changes otherwise people get confused.”ID8
“…I think that is one of the problems that there is still confusion if it falls under infant feeding or acute malnutrition because of the name cMAMI. (…) The very first version of cMAMI was referred to as community-based management of acute malnutrition, and that affords what we call CMAM or IMAM in the community and that would be maybe at sometimes a different team, if you work with government it would be the same health worker but if you are working in like in the refugee context it is slightly different programmatically…”ID8
“I mean helping a mum breastfeeding takes time, you have to be sitting there for 40 min, half an hour, and I think when you do the training, people think oh yeah I understand this, but the actual transition into practice it is quite a big jump there.”ID2
“…is because it builds skills, it builds skills of counsellors because it includes clinical practice, so you learn a skill and then you go out and practice. You learn a new skill you keep building them and then you go out and practice.”ID7
“…like when I was looking for simple tools to do breastfeeding assessment, they weren’t really available, especially not evidence based,”ID1
“...the whole idea of counselling is quite foreign to many of our staff in emergency settings. So because it does take quite of analytical skills, I was thinking of maybe a gap that there is of how do you do a good breastfeeding assessment and then not just doing the assessment but then the next step is okay this is the issue and this is what we are going to address.”ID1
“So I probably say this again one of the main thing is supporting the non-breastfeed, or even relactation so trying to get them back to breastfeeding, and then I think people see it as very complicated with for example wet nursing, (…) from my experience it is actually very challenging to implement because it is not a lot of guidance on it,”ID3
“…it is very rare that I actually find skilled staff who know how to competently give relactation support, but I think as a sector as well we just assume that relactation works and I would actually just throw out there that I have a lot of doubts as to where lactation protocols work.”ID7
“I think we have a tendency to focus on breastfeeding just general recommendation and lactation ahem but when you really dig in to the reasons why women are not succeeding in reaching their goals it comes back down to quite a lot of lactation management problems and issues or lack of support either wasn’t available or did not work (…).”ID7
“I think you need quite highly qualified staff to be able to give that training (…). So, I think my biggest kind of need, but I am not sure that is training per se related, is just a greater clarification and more guidance on how to implement.”ID2
“I just don’t feel we are quite at that point yet where we know how to do it effectively, because I think we are having the right conversations and we are getting the right information together of how to assess and how to report the mothers and if she has mental health problems but I think it is just on the ground where it is not quite working.”ID3
“(…) any other NGO, they don’t have that (…)”, but “Action against Hunger they have mental health and IYCF together, so they have quite a good position that they do that really well (…)(ID3).
Participants voiced a gap in giving trainees the chance to apply and practice newly acquired knowledge, and thus to properly consolidate and refine their skills, in supporting mothers. Training programs were often found to be too theoretical, making it hard for trainees to “transition from abstract training, to how to apply it.”(ID2).
“But you know, it’s only when they actually to talk to mothers or even in the role play that they realise that they are not using the word they should. Like not using judgmental words, but it comes to them and they have (...) and stop themselves from using it, so they only do it if somebody is observing them.”ID9
“Having ongoing mentorship is also really important to be able to follow up and give people support outside of the classroom so I think that should really be considered during implementation.”ID5
“I would say the problems with trainings is that they are given in a very rushed manner when disaster strikes and that is probably not the best, because this is really prevention, with the under six months it should be a preventive measure and it should be in areas which are prone to disasters. For instance, if you have now the Syrian refugees coming to so many countries and people know that they will be coming, so staff should be trained there on the ground to be trained of how to help mothers in how to help them to continue breastfeeding.”ID9
3.2.6. Areas for Improvement: What Would Ideal Training/Support Packages Be Like?
“So again, it is about making the tool comprehensive (…) if you give someone a tool that takes them an hour to read, to document everything and they got 50 patients to see, and one takes an hour, you cannot do it.”ID2
“I don’t think there is a need of new training packages but maybe to go into detail, to some of the topics or modules, that maybe need to be more extended (…)”ID6
“So, to me it is at some point all these things have to come together. You got the early child development, you got to stimulate the child, you got baby WASH, you got to then look at the environment and separate from animals, you got the cMAMI you got to really look at breastfeeding practices and look at the status of the mother. If we think of the end point, of getting a health worker and the health systems delivering this, how can they deliver all of these different packages.ID9
“You know as a range of expertise in the trainer team so you have someone who is an expert and someone who is really quite new to it, but letting them run and be involved in a few trainings and build their confidence and while it is on and if they don’t know the answer, the expert trainer can answer for them, I think that works really well.”ID2
“Just engaging with the materials in lots of different ways, role plays, drill like asking fast questions, sitting and thinking about it, looking at the paper. IMCI does it well, they do lots of different ways, looking at photographs and I think there are lots of different learning styles in a room, so you can kind of compensate all of it and that makes them more comfortable, rather than being forced into a learning style they are not comfortable with.”ID2
“But then I would personally say for things like counselling and mental health it should be like a very practical workshop type. So, I think really technique content needs to be covered for a couple of days and everything else should be very, very practical.”ID3
“One has to prioritise so whoever who is there really needs to know what the setting is like, what the staff who are dealing with these people, what information they already had, what are the other NGOs that are already there, what information, what support they are giving?”ID9
4. Discussion
- Rather than developing completely new additional trainings, future research should focus on how to effectively integrate care of small and nutritionally at-risk infants u6m into future editions of existing training programs available across health and nutrition. The update to Integrated Management of Childhood Illness currently underway by WHO provides one critical opportunity to do so.
- More evidence is needed on how, where, and in what way the training packages we flagged feed into developing heath policies, including policies on breastfeeding support.
- As breastfeeding and relactation support needs are varied and may be complex, more specific training on how to provide this is needed at all stages of a healthcare worker’s career (i.e., undergraduate, postgraduate in-service training, postgraduate formal, and specialist training). Training should include skills in how to effectively re-establish exclusive breastfeeding in at-risk infants u6m and growth outcomes.
- More evidence is needed regarding how to provide health workers without psychological backgrounds with the skills to assess and provide effective mental health counseling.
- Evaluation of the effect of training programs on the quality of services is needed, as well as strategies to sustain quality care provision.
- Training programs should incorporate context-specific practical implementation; the complexity that will limit educational approaches on how best to achieve this requires exploration.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kerac, M.; McGrath, M. 14—Management of Acute Malnutrition in Infants under 6 Months of Age. In The Biology of the First 1000 Days; Karakochuk, C.D., Whitfield, K.C., Green, T.J., Kraemer, K., Eds.; CRC Press: Boca Raton, FL, USA, 2017; pp. 207–220. [Google Scholar]
- Kerac, M.; James, P.T.; McGrath, M.G.; Brennan, E.; Opondo, C.; Frison, S. Infant malnutrition in low- and middle-income countries: Assessment and prevalence of small and nutritionally at-risk infants aged under 6 months in 54 Demographic & Health Survey datasets. medRxiv 2021. [Google Scholar] [CrossRef]
- WHO. WHO Guideline on the Prevention and Management of Wasting and Nutritional Oedema (Acute Malnutrition) in Infants and Children under 5 Year (MAGICapp) 2023. Available online: https://app.magicapp.org/#/guideline/7330 (accessed on 30 July 2023).
- Trowbridge, F.L.; A Sommer, A. Nutritional anthropometry and mortality risk. Am. J. Clin. Nutr. 1981, 34, 2591–2592. [Google Scholar] [CrossRef] [PubMed]
- Pelletier, D.L.; Frongillo, E.A. Changes in Child Survival Are Strongly Associated with Changes in Malnutrition in Developing Countries. J. Nutr. 2003, 133, 107–119. [Google Scholar] [CrossRef]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef] [PubMed]
- Heuvel, M.V.D.; Voskuijl, W.; Chidzalo, K.; Kerac, M.; A Reijneveld, S.; Bandsma, R.; Gladstone, M. Developmental and behavioural problems in children with severe acute malnutrition in Malawi: A cross–sectional study. J. Glob. Health 2017, 7, 20416. [Google Scholar] [CrossRef]
- Kirolos, A.; Goyheneix, M.; Eliasz, M.K.; Chisala, M.; Lissauer, S.; Gladstone, M.; Kerac, M. Neurodevelopmental, cognitive, behavioural and mental health impairments following childhood malnutrition: A systematic review. BMJ Glob. Health 2022, 7, e009330. [Google Scholar] [CrossRef]
- Grey, K.; Gonzales, G.B.; Abera, M.; Lelijveld, N.; Thompson, D.; Berhane, M.; Abdissa, A.; Girma, T.; Kerac, M. Severe malnutrition or famine exposure in childhood and cardiometabolic non-communicable disease later in life: A systematic review. BMJ Glob. Health 2021, 6, e003161. [Google Scholar] [CrossRef]
- Calcaterra, V.; Zuccotti, G. Metabolic, Endocrine, and Cardiovascular Risks in Children with Overnutrition and Undernutrition. Children 2022, 9, 926. [Google Scholar] [CrossRef]
- Mandy, M.; Nyirenda, M. Developmental Origins of Health and Disease: The relevance to developing nations. Int. Health 2018, 10, 66–70. [Google Scholar] [CrossRef]
- Wells, J.C.K. The capacity–load model of non-communicable disease risk: Understanding the effects of child malnutrition, ethnicity and the social determinants of health. Eur. J. Clin. Nutr. 2018, 72, 688–697. [Google Scholar] [CrossRef] [PubMed]
- Black, M.M.; Lutter, C.K.; Trude, A.C.B. All children surviving and thriving: Re-envisioning UNICEF’s conceptual framework of malnutrition. Lancet Glob. Health 2020, 8, e766–e767. [Google Scholar] [CrossRef]
- Management of at Risk Mothers and Infants (MAMI)—Main Website 2021. Available online: https://www.ennonline.net/ourwork/research/mami (accessed on 27 January 2021).
- Kerac, M.; Frison, S.; Connell, N.; Page, B.; McGrath, M. Informing the management of acute malnutrition in infants aged under 6 months (MAMI): Risk factor analysis using nationally-representative demographic & health survey secondary data. PeerJ 2019, 6, e5848. [Google Scholar] [CrossRef]
- Stewart, R.C. Maternal depression and infant growth—A review of recent evidence. Matern. Child Nutr. 2007, 3, 94–107. [Google Scholar] [CrossRef] [PubMed]
- Dadi, A.F.; Akalu, T.Y.; Wolde, H.F.; Baraki, A.G. Effect of perinatal depression on birth and infant health outcomes: A systematic review and meta-analysis of observational studies from Africa. Arch. Public Health 2022, 80, 34. [Google Scholar] [CrossRef]
- WHO. Updates on the Management of Severe Acute Malnutrition in Infants And Children (Guideline) 2013. Available online: https://www.who.int/publications/i/item/9789241506328 (accessed on 27 January 2020).
- Ashorn, P.; Ashorn, U.; Muthiani, Y.; Aboubaker, S.; Askari, S.; Bahl, R.; E Black, R.; Dalmiya, N.; Duggan, C.P.; Hofmeyr, G.J.; et al. Small vulnerable newborns—Big potential for impact. Lancet 2023, 401, 1692–1706. [Google Scholar] [CrossRef] [PubMed]
- Kerac, M.; Angood, C.; McGrath, M.; Lelijveld, N.; Trehan, I.; Manary, M. Towards rollout of new who guidelines for improved management of severe acute malnutrition in infants aged <6 months: An agree appraisal of national guidelines. In Proceedings of the Nutrition & Growth Conference, Amsterdam, The Netherlands, 3 March 2017. [Google Scholar]
- Islam, M.M.; Arafat, Y.; Connell, N.; Mothabbir, G.; McGrath, M.; Berkley, J.A.; Ahmed, T.; Kerac, M. Severe malnutrition in infants aged <6 months—Outcomes and risk factors in Bangladesh: A prospective cohort study. Matern. Child Nutr. 2018, 15, e12642. [Google Scholar] [CrossRef]
- Rana, R.; McGrath, M.; Sharma, E.; Gupta, P.; Kerac, M. Effectiveness of Breastfeeding Support Packages in Low- and Middle-Income Countries for Infants under Six Months: A Systematic Review. Nutrients 2021, 13, 681. [Google Scholar] [CrossRef]
- Grey, K.; Rana, R.; McGrath, M.; Kerac, M. Key considerations for developing patient management tools for small and nutritionally at-risk infants: A scoping review. World Nutr. 2023, 14, 58–75. [Google Scholar] [CrossRef]
- Engler, R. Training Packages and Patient Management Tools for Staff Working with Mothers and Nutritionally At-Risk Infants Aged under 6 Months: A Qualitative Study (MSc Summer Project, LSHTM) 2019. Available online: https://discover.lshtm.ac.uk/permalink/44HYG_INST/od12o/alma991000807713103736 (accessed on 19 August 2023).
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef]
- Palinkas, L.A.; Horwitz, S.M.; Green, C.A.; Wisdom, J.P.; Duan, N.; Hoagwood, K. Purposeful Sampling for Qualitative Data Collection and Analysis in Mixed Method Implementation Research. Adm. Policy Ment. Health Ment. Health Serv. Res. 2015, 42, 533–544. [Google Scholar] [CrossRef] [PubMed]
- Guest, G.; Namey, E.; Chen, M. A simple method to assess and report thematic saturation in qualitative research. PLoS ONE 2020, 15, e0232076. [Google Scholar] [CrossRef]
- Brabandere, A.D.; McGrath, M. HTP v 2 Module 17: Infant and Young Child Feeding: Emergency Nutrition Network (ENN); 2011. Available online: https://www.ennonline.net/htpv2module17 (accessed on 2 July 2023).
- WHO. Breastfeeding Counselling: A Training Course 1993. Available online: https://www.who.int/publications/i/item/WHO-CDR-93.3-5 (accessed on 2 July 2023).
- UNICEF. The Community Infant and Young Child Feeding Counselling Package 2023. Available online: https://www.unicef.org/documents/community-iycf-package (accessed on 2 July 2023).
- WHO/UNICEF. Infant and Young Child Feeding Counselling: An Integrated Course: Trainer’s Guide. Available online: https://www.who.int/publications/i/item/9789240032828 (accessed on 2 July 2023).
- WHO. Handbook: IMCI Integrated Management of Childhood Illness; World Health Organization: Geneva, Switzerland, 2005; Available online: https://apps.who.int/iris/handle/10665/42939 (accessed on 2 July 2023).
- ENN; IBFAN-GIFA; Fondation Terre des Hommes; CARE USA; Action Contre la Faim; UNICEF; UNHCR; WHO; WFP; Linkages. Infant Feeding in Emergencies (IFE) Module 2, Version 1.1 (2007): Emergency Nutrition Network (ENN). Available online: https://www.ennonline.net/ifemodule2 (accessed on 2 July 2023).
- WHO; UNAIDS; UNICEF. HIV and Infant Feeding Counselling: A Training Course. 2000. Available online: https://apps.who.int/iris/handle/10665/66194 (accessed on 2 July 2023).
- WHO. Thinking Healthy: A Manual for Psychosocial Management of Perinatal Depression, WHO Generic Field-Trial Version 1.0, 2015 Turkey: World Health Organization. 2015. Available online: https://apps.who.int/iris/handle/10665/152936 (accessed on 3 July 2023).
- ENN. C-MAMI Tool, Version 2 2018. Available online: https://www.ennonline.net/c-mami (accessed on 11 April 2021).
- LSHTM. Getting to Know Cerebral Palsy: Working with Parent Groups—A Training Resource for Facilitators, Parents, Caregivers, and Persons with Cerebral Palsy. 2014. Available online: https://medbox.org/document/getting-to-know-cerebral-palsy-display-materials#GO (accessed on 3 July 2023).
- Save the Children. Infant and Young Child Feeding in Emergencies (IYCF-E) Toolkit: Rapid start-up for emergency nutrition personnel | Save the Children’s Resource Centre 2021. Available online: https://resourcecentre.savethechildren.net/document/infant-and-young-child-feeding-emergencies-iycf-e-toolkit-rapid-start-emergency-nutrition (accessed on 3 July 2023).
- ACF. Baby Friendly Spaces: A Technical Manual | Action Against Hunger 2014. Available online: https://www.actionagainsthunger.org/publications/baby-friendly-spaces-technical-manual (accessed on 2 July 2023).
- HOLT. Feeding & Positioning Manual: Guidelines for Working with Babies and Children 2019. Available online: https://www.holtinternational.org/nutrition-health/feeding-positioning-manual (accessed on 2 July 2023).
- CARE; URC; CHS. Infant and Young Child Feeding Counselling a Community-Focused Approach Trainer’s Guide | Food Security and Nutrition Network 2023. Available online: https://www.fsnnetwork.org/resource/infant-and-young-child-feeding-counselling-community-focused-approach-trainers-guide (accessed on 2 July 2023).
- MAMI Global Network; ENN; LSHTM. MAMI Care Pathway Package, Version 3. 2021. Available online: https://www.ennonline.net/mamicarepathway (accessed on 16 May 2021).
- Gavine, A.; MacGillivray, S.; Renfrew, M.J.; Siebelt, L.; Haggi, H.; McFadden, A. Education and training of healthcare staff in the knowledge, attitudes and skills needed to work effectively with breastfeeding women: A systematic review. Int. Breastfeed. J. 2016, 12, 6. [Google Scholar] [CrossRef] [PubMed]
- Grey, K.; Brennan, E.; Kerac, M.; McGrath, M. The MAMI Care Pathway Package: A resource to support the management of small and nutritionally at-risk infants under six months of age and their mothers (MAMI). South Sudan Med. J. 2021, 14, 94–97. [Google Scholar] [CrossRef]
- Menon, P.; Covic, N.M.; Harrigan, P.B.; Horton, S.E.; Kazi, N.M.; Lamstein, S.; Neufeld, L.; Oakley, E.; Pelletier, D. Strengthening implementation and utilization of nutrition interventions through research: A framework and research agenda. Ann. N. Y. Acad. Sci. 2014, 1332, 39–59. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, S.; Menon, P.; Kennedy, A.L. Scaling Up Impact on Nutrition: What Will It Take? Adv. Nutr. Int. Rev. J. 2015, 6, 440–451. [Google Scholar] [CrossRef]
- Rea, M.F.; I Venancio, S.; Martines, J.C.; Savage, F. Counselling on breastfeeding: Assessing knowledge and skills. Bull. World Health Organ. 1999, 77, 492–498. [Google Scholar]
- Zakarija-Grković, I.; Burmaz, T. Effectiveness of the UNICEF/WHO 20-hour Course in Improving Health Professionals’ Knowledge, Practices, and Attitudes to Breastfeeding: A Before/After Study of 5 Maternity Facilities in Croatia. Croat. Med. J. 2010, 51, 396–405. [Google Scholar] [CrossRef]
- Mitchell, J. Health in Emergencies Learning in Humanitarian Assistance 2 Current Debates Learning in the Field Learning from Teaching Learning through Evaluation Eha Regional Contacts. The New Humanitarianism: Challenges for Emergency Health Sector to Improve Learning and Competency. 2003. Available online: www.alnap.org (accessed on 2 July 2023).


{kind=link}
| A | B | C | D | E | F | G | H | I | J | K | L | M | N | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Curriculum Covered | Harmonised Training Package (HTP) [28] | Breastfeeding Counselling a Training Course [29] | Community IYCF Counselling Pack [30] | IYCF Counselling: an Integrated Course [31] | IMCI [32] | Infant Feeding in Emergencies “Module 2” [33] | HIV Infant Feeding Counselling [34] | Think Healthy [35] | cMAMI Tool (v.2) [36] | Getting to Know Cerebral Palsy [37] | IYCF-E Toolkit [38] | Baby Friendly Spaces [39] | Feeding + Positioning Manual [40] | IYCF Counselling Community-Focused Approach [41] |
| Infant | ||||||||||||||
| Feeding Assessment | X | X | X | X | X | X | X | X | X | X | ||||
| Anthropometry/Nutritional Assessment | X | X | X | X | ||||||||||
| The Sick Child | X | X | X | |||||||||||
| LBW Babies | X | X | X | X | X | X | X | X | X | X | ||||
| Breastfeeding | X | X | X | X | X | X | X | X | X | X | X | X | X | |
| Relactation | X | X | X | X | X | |||||||||
| Mother | ||||||||||||||
| Health Assessment | X | X | X | X | X | |||||||||
| Nutrition, Physical Health | X | X | X | X | X | X | X | X | X | X | ||||
| HIV and Infant Feeding | X | X | X | X | X | X | X | X | X | X | ||||
| Disability | X | X | ||||||||||||
| Counselors | ||||||||||||||
| Counseling Skills | X | X | X | X | X | X | X | X | X | X | X | |||
| Communication Skills | X | X | X | X | X | X | X | X | X | |||||
| Other | ||||||||||||||
| Management of Artificial Feeding/Donations | X | X | X | X | X | |||||||||
| Emergency Preparedness | X | X | X | X | ||||||||||
| Integration into Other Nutrition Programs | X | X | X | X | ||||||||||
| Food Hygiene | X | X | X | X | ||||||||||
| Participant ID | Organization Type | Setting |
|---|---|---|
| 1 | NGO | Outpatient Care |
| 2 | Academic/Research Institution | Inpatient Care |
| 3 | NGO | Emergencies |
| 4 | Hospital | Inpatient Care |
| 5 | NGO | In- and Outpatient Care |
| 6 | NGO | Community Setting |
| 7 | NGO | Inpatient Care |
| 8 | NGO | Community Setting |
| 9 | Nutrition Initiative | Emergencies |
| ID | Training Used | Setting | Target Audience | Duration | Costs | Curriculum | Guidelines Followed |
|---|---|---|---|---|---|---|---|
| 1 | cMAMI | Emergencies, communities | IYCF counselors, nurses | 2 days on cMAMI, 3-day IYCF plus 2 days and then once a week | No direct costs or travel costs for staff | Save the Children IYCF training | Modified from cMAMI guidance, national guidelines, WHO |
| 2 | IMCI, IYCF, cMAMI | Hospital, communities | CHW, IMCI: doctors, nurses, paramedics | 3 to 5 days, IMCI and IYCF often running for 3 to 4 months in inpatient | N/A | IMCI curriculum, IYCF curriculum, breastfeeding | IYCF, FANTA |
| 3 | IYCF, IYCF-E, cMAMI | Emergencies | IYCF counselors, managers, trainers | 5 days for managers, for counselors usually 3 days | Venue, food during trainings, material, baby dolls, relactation kit | IYCF-E curriculum, relactation, exclusive BF, topics related to <6 months, counseling skills, setting up an artificial feeding program, psychosocial support, staffing | WHO, UNICEF |
| 4 | Tailor-Made Course | Hospital | HW, doctors, nurses, nutritionists, peer supporters | 5 days | N/A | Pathology of malnutrition, clinical management of malnutrition | Baby-friendly hospital initiative, national guidelines for management of acute malnutrition |
| 5 | Neonatal Feeding Training | Inpatient clinic | Nurses, social workers/HW with different backgrounds, midwives | 5 days | N/A | Assessment, diagnosis, treatment, what is good BF: how many times a day, breastfeeding assessment, counseling, monitoring | National guidelines, malnutrition guidelines from WHO, UNICEF, FANTA |
| 6 | Community IYCF Counseling Pack | Community | Nutrition officers, protection officers, community mobilisers, nutrition coordinators | 3 to 5 days | N/A | Community awareness, community sensitization, content for under six months | WHO, UNICEF |
| 7 | 40h Breastfeeding Course, Tailor-Made Course, Infants With Feeding Difficulties | Inpatient | Front-line community workers, healthcare staff | 5 days | N/A | ||
| 8 | cMAMI | Emergencies | Nurses with nutrition experience | 1 to 3 days | N/A | cMAMI toolkit, national guidelines | |
| 9 | Training Based on WHO, UNICEF and Later Modified Version, IYCF-E | Emergencies | Variety off people with different backgrounds | Depending on setting and resources | N/A | Growth monitoring, taking anthropometrics |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Engler, R.; McGrath, M.; Kerac, M. Training Packages and Patient Management Tools for Healthcare Staff Working with Small, Nutritionally At-Risk Infants Aged under 6 Months: A Mixed-Methods Study. Children 2023, 10, 1496. https://doi.org/10.3390/children10091496
Engler R, McGrath M, Kerac M. Training Packages and Patient Management Tools for Healthcare Staff Working with Small, Nutritionally At-Risk Infants Aged under 6 Months: A Mixed-Methods Study. Children. 2023; 10(9):1496. https://doi.org/10.3390/children10091496
Chicago/Turabian StyleEngler, Ramona, Marie McGrath, and Marko Kerac. 2023. "Training Packages and Patient Management Tools for Healthcare Staff Working with Small, Nutritionally At-Risk Infants Aged under 6 Months: A Mixed-Methods Study" Children 10, no. 9: 1496. https://doi.org/10.3390/children10091496