




by
, , , , , , and

Curr. Oncol. 2023, 30(9), 8117-8133; https://doi.org/10.3390/curroncol30090589 (registering DOI) - 01 Sep 2023
Abstract
(1) Background: Several studies have investigated potential interactions between immune checkpoint inhibitors (ICIs) and commonly prescribed medications. Although acetaminophen (APAP) has not been considered susceptible to interaction with ICIs, recent research has shown that detectable plasma levels of this drug can hinder the
[...] Read more.
(1) Background: Several studies have investigated potential interactions between immune checkpoint inhibitors (ICIs) and commonly prescribed medications. Although acetaminophen (APAP) has not been considered susceptible to interaction with ICIs, recent research has shown that detectable plasma levels of this drug can hinder the efficacy of PD-1/PD-L1 blockade therapies. A reliable assessment of the potential interaction between APAP and ICIs in advanced non-small cell lung cancer (NSCLC) patients would be worthwhile since it is often prescribed in this condition. We sought to evaluate the impact of the concomitant use of APAP in patients with advanced NSCLC on PD-1/PD-L1 blockade using real-world evidence. (2) Methods: This study included consecutive patients with histologically proven stage IV NSCLC who underwent first-line therapy with pembrolizumab as a single agent or in combination with platinum-based chemotherapy, or second-line therapy with pembrolizumab, nivolumab, or atezolizumab. The intensity of APAP exposure was classified as low (therapeutic intake lasting less than 24 h or a cumulative intake lower than 60 doses of 1000 mg) or high (therapeutic intake lasting more than 24 h or a total intake exceeding 60 doses of 1000 mg). The favorable outcome of anti-PD-1/PD-L1 therapies was defined by durable clinical benefit (DCB). Progression-free survival (PFS) and overall survival (OS) were relevant to our efficacy analysis. Propensity score matching (PSM) methods were applied to adjust for differences between the APAP exposure subgroups. (3) Results: Over the course of April 2018 to October 2022, 80 patients were treated with first-line pembrolizumab either as single-agent therapy or in combination with platinum-based chemotherapy. During the period from June 2015 to November 2022, 145 patients were given anti-PD-1/PD-L1 blockade therapy as second-line treatment. Subsequent efficacy analyses relied on adjusted PSM populations in both treatment settings. Multivariate testing revealed that only the level of APAP and corticosteroid intake had an independent effect on DCB in both treatment lines. Multivariate Cox regression analysis confirmed high exposure to APAP and immunosuppressive corticosteroid therapy as independent predictors of shorter PFS and OS in both treatment settings. (4) Conclusions: Our findings would strengthen the available evidence that concomitant intake of APAP blunts the efficacy of ICIs in patients with advanced NSCLC. The detrimental effects appear to depend on the cumulative dose and duration of exposure to APAP. The inherent shortcomings of the current research warrant confirmation in larger independent series.
Full article
(This article belongs to the Special Issue Immunotherapy in Thoracic Malignancies)
►
Show Figures
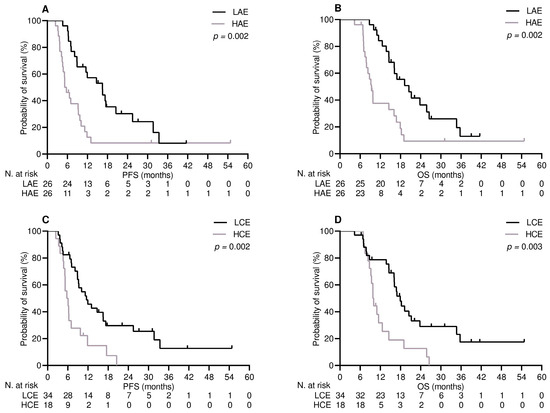
Figure 1












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}